
The Athlete
Drug Abuse
Alcohol Problems
SELF-MEDICATION & MENTAL PROBLEMS
Often alcohol is drunk because the person has an existing mental problem such as major depression, schizophrenia, bipolar illness (manic-depression), or panic disorder. The person uses alcohol to try to control the symptoms or to avoid asking for psychiatric help.
"I would pick up some beer to put me out of it. I didn't like the effect that regular psychiatric drugs, such as antidepressants, had on my brain and I'd rather just put myself out with the booze."
Patient with major depression and an alcohol problem
Sometimes alcohol is used for other reasons-to overcome boredom or control restlessness. Unfortunately what happens is that the attempt to self-medicate by drinking can take on a life of its own and create a new set of problems or aggravate an existing one. For example, a person may use alcohol to escape depression although chronic alcohol abuse may actually contribute to depression (Miller, Klamen, Hoffman, & Flaherty, 1995). A study of adults with panic disorder showed that the subjects reported significantly less anxiety and fewer panic attacks when drinking. The use of alcohol to control the symptoms resulted in a higher rate of alcohol use disorders among those with panic disorder (Kushner, Mackenzie, Fiszdon, et al., 1996).
"The problems did get worse when I was drinking. That was one reason that I never figured out I was a manic-depressive. I figured I was depressed because I was drunk all the time."
Alcoholic with manic-depression
Alcoholics are
- 21 times more likely to have an antisocial personality disorder,
- 3.9 times more likely to have a drug abuse disorder, L 6.2 times more likely to have manic depressive disorder,
- 4 times more likely to have schizophrenia. (Helzer & Pryzbeck, 1988)
The majority of alcoholics who come into treatment are initially diagnosed as suffering from depression. In addition about 1/3 of alcoholics suffer an anxiety disorder.
| Table 5-4. Some alcohol-related causes of death | ||
| Diseases (indirectly caused by alcohol) |
Diseases (indirectly caused by alcohol) |
Injuries/adverse effects (indirectly caused by alcohol) |
| Alcoholic psychoses Alcoholism Alcohol abuse Nerve degeneration Heart disease Alcoholic gastritis Fatty liver Hepatitis Cirrhosis Other liver damage Excessive BAC Accidental poisonings Seizure activity |
Tuberculosis Cancer of the lips, mouth, and pharynx Cancer of the larynx, esophagus, stomach, and liver Diabetes Hypertension Stroke Pancreatitis Diseases of stomach, esophagus, and duodenum Cirrhosis of bile tract |
Boating accidents Motor vehicle, bicycle, other road accidents Airplane accidents Falls Fire accidents Drownings Suicides, self-inflicted injuries Homicides or shootings Choking on food Domestic violence Rapes or date rapes |
| (Adapted from U.S. Department of health and Human Services, Alcohol and Health, 1997) | ||
"The alcohol, that came later on. It intensified my depression and intensified everything. I already felt bad about myself and the alcohol just made it worse. It definitely made it worse."
Researchers from the Scripps Institute found that heavy drinking strips the brain of its natural chemical reactions that trigger feelings of well-being in the mesolimbic/dopinergic reward pathway (opioid peptides, dopamine, serotonin, and GABA) while raising the levels of chemicals that cause tension and depression, including norepinephrine, epinephrine, and serotonin (Koob, 1999). The brain tries to compensate for the depletion of neurotransmitters by releasing corticotropin-releasing factor, a stress chemical that, unfortunately, can induce depression. The depression can last for as long as a month after abstinence begins. This combination of decreased action of reward chemicals and excess stress chemical increases craving for alcohol.
MORTALITY
Drinking can affect a person's life span since heavy drinking increases the chances of dying from disease or trauma. For instance, the average life span is shortened 4 years by cancer, 4 years by heart disease, and from 9-22 years for alcoholic liver disease. In one study a difference in life span was found even between abstainers (defined as 12 drinks or less per year) and light drinkers (1-2 drinks per day) (Vaillant, 1995; U.S. Department of Health & Human Services, 1997).
FETAL ALCOHOL SYNDROME (FAS) & FETAL ALCOHOL EFFECTS (FAE)
Maternal Drinking
A survey of pregnant women in the United States found that 18.8% drank alcohol during pregnancy while 5.5% used illicit drugs at least once (NIDA, 1996). Alcohol use during pregnancy is the leading cause of mental retardation in the United States (Abel & Sokol, 1986; Cook et al., 1991). Alcohol overuse during pregnancy also increases the number of miscarriages and infant deaths; there are more problem pregnancies; and newborns are smaller and weaker. Certain specific toxic effects of alcohol on the developing fetus are known as "fetal alcohol syndrome" or FAS, a term first coined in 1973 (Jones & Smith, 1973). At first it was thought that the defects were the result of malnutrition but the toxicity of alcohol was recognized as the cause. Criteria for standardizing the diagnosis of FAS were standardized in 1980. The defects can range widely from obvious gross physical defects to behavioral problems. Not all women who drink heavily during pregnancy bear children with FAS. There is as yet no definitive test for confirming FAS at birth and only the most severe cases are diagnosable at birth.

The greatest danger of alcohol use by a pregnant woman is brain damage. The larger brain on the left is the normal brain of a human newborn (that died in an accident). The smaller brain on the right is of a child born with FAS or fetal alcohol syndrome. The FAS brain is obviously small and malformed. Often the damage is more subtle and learning deficits don't show up until the children are six or seven years old. Courtesy of Sterling K. Clarren, MD, Children's Hospital, Seattle
The minimal standards for a diagnosis of FAS are
- retarded growth before and after birth, including height, weight, head circumference, brain growth, and brain size;
- central nervous system involvement such as delayed intellectual development, neurological abnormalities, behavioral problems, visual problems, hearing loss, and balance or gait problems;
- facial deformities including shortened eye openings, thin upper lip, flattened midface, groove in the upper lip, and occasional problems with heart and limbs. (Sokol & Clarren, 1989)
In addition children with FAS are liable for increased risks of other common birth defects including heart disease, cleft lip and palate, and spina bifida. A weak and irregular sucking response, jitteriness, trembling, and sleep disturbances have been reported in babies exposed to large doses of alcohol. If only a few of these FAS attributes are present, the diagnosis could be fetal alcohol effect (FAE) or alcohol-related birth defects (ARBD) (NIAAA, 1997). Worldwide studies estimate that FAS births occur anywhere from 0.33 to 2.9 cases per 1,000 live births. In the United States, African Americans have about 6 FAS births per 1,000; Asians, Hispanics, and Whites, about 1 to 2; and Native Americans about 30, although rates from 10-120 births per 1,000 have been reported in various specific Native American and Canadian Indian communities. FAE rates are 1.7 to 3.6 while ARBD rates range from 3.4 to 6.0 (May, 1996; Hans, 1998).
Critical Period. Because the brain is among the first organs to develop and the last to finish, it appears to be vulnerable throughout pregnancy, however weeks three through eight, at the onset of embryogenesis (formation of the embryo), are crucial. For example, the corpus callosum, a crucial structure that connects the cerebral hemispheres, is extremely vulnerable to alcohol use during the sixth to eighth gestational weeks; damage to the basal ganglia affects fine motor coordination and cognitive ability (Rosenberg, 1996). The greatest behavioral damage results from early heavy fetal exposure to alcohol.
Critical Dose. Animal models suggest that peak blood alcohol concentration rather than the total amount of alcohol drunk determines the critical level above which adverse effects are seen. A pattern of rapid drinking and the resulting high BAC seem to be the most dangerous style of drinking.
How many drinks are safe during pregnancy? One study concludes that seven standard drinks per week by pregnant mothers are a threshold level below which most neurobehavioral effects are not seen. This might lead some health care professionals to feel that they need not recommend total abstinence. However seven drinks per week are an average and if a pregnant woman consumes a large number of those drinks at one sitting, the fetus may be much more at risk. Also some neurobehavioral tests are so sensitive that effects on the fetus can be found even with extremely low levels of exposure to alcohol. Further it is important to remember that even one drink per day has been associated with the development of breast cancer in women.
A new animal study showed that even one high-dose use episode of alcohol in rats, when the developing brain is creating neurons and neuronal connections at a furious pace, will also kill brain cells at a furious pace. In the experiment they showed that normally 1.5% of brain cells die during a certain period in a rat's growth but in rats exposed to alcohol during that critical period, 5% to 30% of neurons will die. When extrapolating these results to humans, the blood alcohol concentration would be .20, about twice the legal allowable limit for drivers and the crucial period would be six months into the pregnancy until two years after birth. During the brain growth spurt, a single prolonged contact with alcohol lasting for four hours or more is enough to kill vast numbers of brain cells (Ikonomidou, Bitigau, Ishimaru, et al., 2000).
One approach suggests that one standard drink every 10 days might be safe but there is still the potential for unobservable damage that could impair a child when stressed or when the child reaches adulthood and old age. The U.S. Surgeon General advises that pregnant women should not drink at all while pregnant since there is no way to determine which babies might be at risk from even very low levels of alcohol exposure. Current research simply does not permit us to know at what quantity alcohol begins to damage the fetus (Ernhart, Sokol, Martier, et al., 1987; NIAAA, 1997; Hans, 1998).
Paternal Drinking
Genetic transmission of alcoholism by fathers is strongly suspected. There is now growing evidence that the detrimental effects of alcohol on the fetus may also be transmitted by paternal alcohol consumption. Researchers are unable to say definitively whether paternal exposure to alcohol results in FAS or in some other syndrome. In laboratory tests, alcoholic-sired rats of nonalcohol-using mothers produced male offspring with disturbed hormonal functions and spatial learning impairments. Adolescent male rats subjected to high alcohol intake produced both male and female offspring suffering from abnormal development.
Observations of alcoholic-sired human males indicate no gross physical deficits but do show an association with intellectual and functional deficits in offspring. In addition to the deficits in verbal, thinking, and planning skills of children of alcoholics (COAs), sons of male alcoholics (SOMAs) exhibit further deficiencies in visual/spatial skills, motor skills, memory, and learning (NIAAA, 1997).
Preliminary explanations of the causes of these abnormalities suggest that alcohol may mutate genes in sperm, kill off certain kinds of sperm, or biochemically and nutritionally alter semen and influence sperm.
ADVERSE SOCIAL CONSEQUENCES
Aggression & Violence
"On a typical Friday night, at least 50% of our calls will be some kind of alcohol and drug violent behavior situation whether it be a shooting, stabbing, or a beating. A lot of those involve significant others, a spouse, or cohabitants."
Emergency medical technician, San Francisco, 1997
In the past 15 years almost every major league baseball park and professional football stadium has stopped selling beer in the spectator seats. Alcohol and beer must now be purchased only at the concession stands where a customer is limited to two drinks at a time and no sales are allowed after the seventh inning or third quarter. These changes have sharply reduced rowdiness, violence, and fights. In England and other countries where such a ban is rare, fan violence, especially at soccer matches, is still a major problem.
Alcohol itself usually does not cause a person to be violent but it can magnify existing traits and susceptibility and contribute to or trigger interpersonal and criminal violence.
"The use of alcohol would really bring out the hit man in me. I mean, I could talk to my partner or whoever fairly good if I was sober but after I started drinking, the deep emotions really would come out."
28-year-old male in domestic violence prevention class
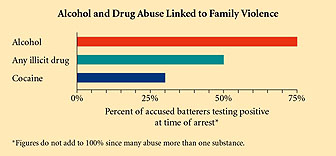
Figure 5-7. Three out of four of those arrested for family violence tested positive for alcohol. Half had used some illicit drug and more than one in four tested positive for cocaine. The National Research Council, 1993
Based on victim reports, 15% of robberies, 27% of aggravated assaults, 50% of all homicides, and 37% of rapes and sexual assaults involved alcohol use (U.S. Department of Justice, 1998; Roizen, 1997). About 1/3 of the 5.3 million convicted offenders under the jurisdiction of corrections agencies in 1996 were drinking at the time of their offense. There are some relatively fixed and unalterable pharmacological causal connections between alcohol and violence. Alcohol has been shown to increase aggression by interfering with GABA, the main inhibitory neurotransmitter, in ways that may encourage intoxicated people with preexisting aggressive tendencies to become aggressive. Also, in some people alcohol can increase dopamine, which stimulates aggression. Alcohol also decreases the action of serotonin that may cause drinkers to use aggression to gain pleasure and avoid punishment and to be less able to stop drinking once it has started (Gustafson, 1994).
There are also some variable causes of alcohol-related violence that are complex and involve personality, occasion (setting), social and cultural factors, and economic conditions. Experiments have shown that the expectation that alcohol will make one braver leads people to be more aggressive even if they are drinking a nonalcoholic beverage that they believe contains alcohol (Bushman, 1997). Also, along with increases in the divorce rate, more women are victims of alcohol-influenced homicides.
Because alcohol reduces inhibitions, it can encourage someone with a tendency toward violence to release pent-up anger, hatred, and desires forbidden by society, and to act on them. Besides the homicides and rapes that occur each year due to alcohol, over seven million other crimes are committed under the influence. Alcohol can also undermine moral judgment and increase aggression. When a person drinks, the common sense that would keep a person out of trouble is often suppressed (Collins & Messerschmidt, 1993).
"Seems like alcohol is always referred to as this liquid courage, you know. And I guess it depends where you're at-courage to do what? Courage to ask a girl on a date that you hadn't had the courage to do before, or courage to dance like a fool on the floor, or is it courage to beat your wife or to beat your girlfriend cause you didn't have the guts to do it before?"
College counselor
Another mechanism that connects alcohol and violence is that alcohol can cause a drinker to misjudge social cues causing a person to perceive a threat where none exists. What occurs is that alcohol disrupts the judgment and reasoning center of the brain (Miczek, 1997). In some men alcohol can release their aggressive tendencies and they become violent when they drink but the violence was sitting in them and residing in their psyche way before they picked up that first drink.
"He beat me only when he was drunk. To me it was just an excuse, it was just an excuse of being drunk and doing it. So for me drinking and being violent is just an excuse. It is a coward that is doing it the way I'm seeing it."
43-year-old ex-wife of an alcoholic abuser
Serious & Fatal Injuries
Medical examiner reports indicate that alcohol increases the risk of injury.
- Emergency room studies confirm that from 15% to 25% of emergency room patients tested positive for alcohol or reported alcohol use, with relatively high rates among those involved in fights, assaults, and falls.
- Alcoholics are 16 times more likely than others to die in falls and 10 times more likely to become burn or fire victims.
- The Coast Guard reported that 31% of boating fatalities had a BAC of .10 or more.
- At work up to 40% of industrial fatalities and 47% of injuries involved alcohol. (Bernstein & Mahoney, 1989; NCADI, 1999)
Motor Vehicle Accidents
"Drunken driver Henri Paul caused the 1997 car crash that killed Princess Diana, French judges ruled Friday in a report clearing photographers and her companion Dodi al Fayed of blame for the fatal accident. The 32-page ruling on the high-speed crash said Paul was inebriated and was taking anti-depressants and consequently lost control of the limousine."
Reuters News Service, September 04, 1999
Whether it is the death of the Princess Diana or the death of 27 children in a school bus, drunk driving affects more than just the driver. According to the U. S. National Highway Traffic Safety Administration (NHTSA), more than one in four drivers get behind the wheel within two hours of drinking. This leads to relatively high rates of alcohol use for drivers involved in motor vehicle collisions.
- In one study more than 38% of motor vehicle fatalities in 1997 involved alcohol use. L Alcoholics are five times more likely to die in motor vehicle crashes.
- Projections are that 3 out of every 10 persons in the United States will in some way be involved in an alcohol-related crash during their lifetime.
- On any weekend night 3 out of every 100 drivers exceed the legal BAC limit.
- Of those convicted of DWI, 61% drank beer only, 2% drank wine only, 18% drank liquor only, and 20% drank more than one type of alcoholic beverage.
- About 40% of first-time DUI offenders and 60% of multiple DUI offenders reported consuming five or more drinks compared with 10% of the adult male population.
- Approximately 1 in 7 intoxicated drivers who were involved in a fatal collision had a prior DWI (driving while intoxicated) conviction whereas only 1 in 34 sober drivers involved in a fatal collision had a prior DWI conviction. (NHTSA, 1999, 1998, 1997, 1995; NIAAA, 1997)
Suicide
Among adult alcoholics, sui-cide rates are twice as high as for the general population and from 60-120 times greater than the nonmentally ill population-rates increase with age. One reason given for the increase in suicide with age is that the longer the alcoholism, the more social, health, and interpersonal problems there are. The alcoholic suicide victim is typically white, middle-aged, male, and unmarried with a long history of drinking. Additional risk factors for suicide include depression, loss of job, living alone, poor social support, other illnesses, and continual drinking.
Information on Drug Abuse:
Information on Alcohol:
Epidemiology of Alcohol Consumption